
April 10, 2013

Groin pain is the hardest diagnosis in medicine. The groin is not a muscle, but refers to the crease at the junction of the torso and the thigh. The anatomy looks like the Los Angeles freeway system; lots of on and off-ramps, major highways and minor frontage roads. To make matters more difficult, organs like the intestines or even genitals can also cause pain in this region.
So before we even talk about the occurrence or treatment process, we have to be clear on what a groin injury really is.
What is a Groin Injury?
Our injury process always begins with the critical question of onset.
Did the pain start all of a sudden or has it been bothering you for awhile?
This puts the groin pain into 2 major categories, acute or overuse. In the overuse condition, pain comes/goes with no clear date of onset. This overuse condition generally occurs when the hip joint is in the wrong place (impingement) and has been found in 90% of athletes! This wear and tear condition usually involves lower back pain as well.
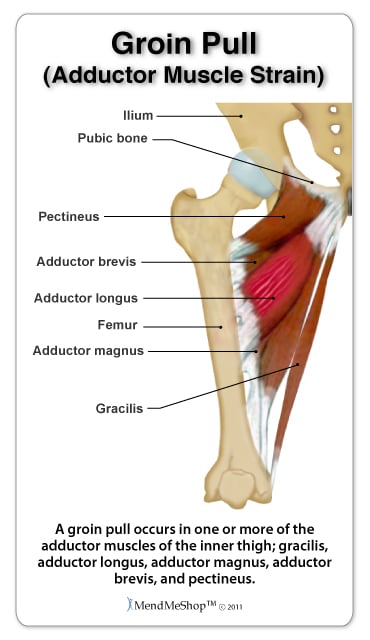
In the case of acute groin pain, you can clearly identify when the injury happened. For example, it could be a “pop”, a specific movement or incident where something felt like it just snapped. This acute groin pain is an adductor muscle strain. The adductors of the hip joint include 6 muscles: the adductor longus, magnus and brevis, along with the gracilis, obturator externus and pectineus.
Sprinters Do Not Have Adductor Strains
Sports with rapid changes of direction are the most likely to have adductor strains, ruling out track athletes who only have to run straight ahead. These sports require a strong eccentric contraction of the adductor musculature, particularly emphasized in quicker sports such as hockey and soccer.
A 2012 review examined predictive tools for several common lower body injuries, including these adductor strains. The authors found that adductor muscle strength was associated with the injury. However, it is not the sheer strength of the adductor muscles. Rather it is the ratio, the strength of the adductors compared with the muscles on the outside of the leg, the abductors. The abductors of the hip are the tensor fasciae latae (TFL) and the glute muscles. When the hip adduction strength was 80% or less of abduction strength, athletes were 17x more likely to have a muscle strain!
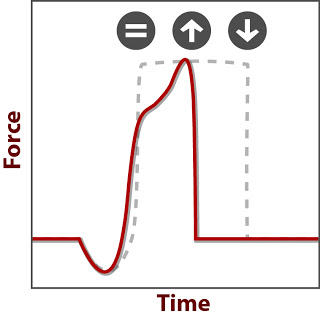
Fortunately, there is an even better method to assess adductor/abductor balance, using the force plate and your Movement Signature. Athletes with over-powerful abductors, which make adductors seem weak, will have high peak forces, EXPLODE. They are just exceptional at being quick and not leaking any force.
The downside to high EXPLODE is the struggle to prolong a movement, such as full extension seen in longer stride lengths. So like hamstring strains, and any soft tissue strain, athletes with a flexed Movement Signature are at risk for adductor strains. The main difference between these injuries is the primary type of movement. More sprinting straight ahead will lead to hamstring strains while more change of direction will lead to adductor strains.
Solution
Regen – Starting with this aspect because the mechanism of injury is directly related to the eccentric stress, the sudden lengthening of the muscle. The adductors need to be lengthened again to avoid reinjury.
Skill – Wall Sit is a great substitute for the normal quick, changes of direction normally focused on for skills. We squeeze an implement between the knees as well to strengthen the adductors simultaneously.
Strength – All muscular strains share a common theme, lack of eccentric strength. So prescribing movements that emphasize the DRIVE portion of your movement signature is critical. The added bonus of prescribing leg curl is the stimulus of your hamstrings as hip extensors rather than the adductor magnus.
So if you can identify the exact time groin pain started, it is an adductor strain. Silence your TFL and get to work on DRIVING better.
References
Dallinga JM, Benjaminse A, Lemmink KA. Which screening tools can predict injury to the lower extremities in team sports?: a systematic review. Sports Med. 2012 Sep 1;42(9):791-815.