
August 8, 2018

When rehabilitating injuries, both in sports medicine and more traditional medical settings, somehow extremely subjective functional testing is still the standard. In fact, it is not uncommon for a doctor or therapist to make assumptions based off the classic “push into my hand” test.
Just think about that for a second.
While it is easy to trust anyone in a white coat, we should really be looking into how things are measured and assessed. With over 650,000 (and counting) standardized assessments in our database, we have seen the power of using a force plate as an objective diagnostic and assessment tool to take a leap forward in a world where subjective tests have long been the unquestioned norm.
The same cookie cutter rehab protocols are often used on all populations regardless of individual differences, such as age, ethnicity, gender, training history, etc. These protocols are often time based, developed from the average time taken for tissue to heal, which clearly isn’t the same for each individual. For that reason, it’s imperative to look at rehab through an objective lens to decide when to push (pun intended) forward, or pull the reins on current rehab practice. More importantly, it’s paramount to understand that this isn’t about you. It’s about those we serve (patients, athletes,soldiers) who depend on us to get them back to performing at optimal levels.
Best practice for creating an objective rehab plan is establishing a baseline on each patient early (and often). Like any assessment, frequent monitoring tends to improve understanding on a deeper level – by getting a baseline number on both the Balance and Plank Scans (proprioception and static stability) you can have a reference point to compare to in case of future injury. The practicality of these assessments allows for testing to be frequent, as “baseline” tests from six months ago are rarely (if ever) valid today. Not only will this information validate the progress seen by the practitioner, but in my experience – it helps to have everyone involved speaking the same language. If the surgeon, physical therapist, and strength and conditioning professional are on the same page in terms of recovery, it allows the process to run much smoother. Being able to track progress without relying on subjective measures is not only critical for the alignment and cooperation of those involved, but for the success of the individual, who should have full transparency in the rehabilitation process as well.
What is the Balance Scan measuring?
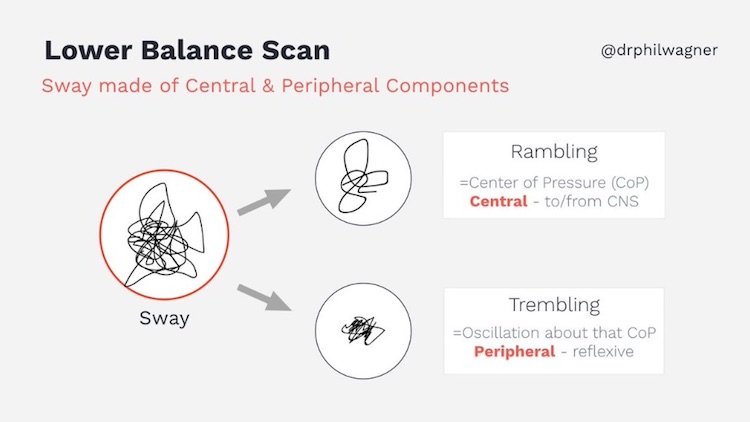
Average Sway Velocity – a measure of the center of pressure (CoP) path distance over trial time
Higher scores are indicative of the individual’s ability to display control of their CoP with smaller deviation (such as rambling/trembling that is shown above) – which is a measure of sensorimotor control and functional stability. Lower scores would show the opposite, an instability or lack of control, which has shown to have implications of injury or reinjury when below 48 for each limb. What you are really looking at after injury (including concussion) is potential loss of stability, coordination, or proprioception (body awareness).
Inadequate levels of these qualities could put the patient back on the training table. Does the individual show enough stability to control the limbs/body? Do they have the awareness to quickly correct when they become off balance? If you’re guessing here, you need to rethink your process.
Utilizing a non-invasive test like the Balance Scan is especially important in the precious days immediately following the injury. Being able to refer back to baseline scores, or benchmarks for proprioception and motor control is extremely helpful. However, frequent and practical assessment can help advance the rehabilitation process at a quicker (and more objective) pace than most time-based protocols. It is not uncommon to see our partners assessing balance post injury up to 3 times per week.
Once the subject has demonstrated adequate static stability, or at least show headway comparable to their baseline numbers, it is reasonable to move forward toward more dynamic assessments such a jumping tasks. Not only can this lead to shorter rehabilitation timelines, but it also gives the individual a sense of responsibility and autonomy for their advancement, which increases motivation and engagement. Utilizing objective functional testing to track patient progress can make all the difference in effort seen, and in return the success of both patient and practitioner.